
Case Studies
- Home
- Media
- Case Studies
Rigid Bronchoscopy – Cryobiopsy of Protruding Mass – Endobronchial Blocker(Fogarty Balloon)
Background
60 year old alcoholic and diabetic patient presented with complaints of fever, cough, loss of appetite and loss of weight.
Diagnosis And Treatment
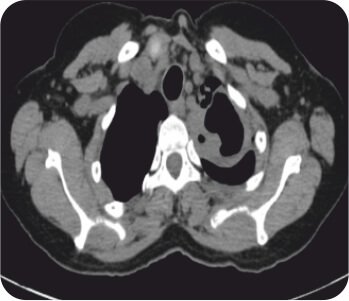
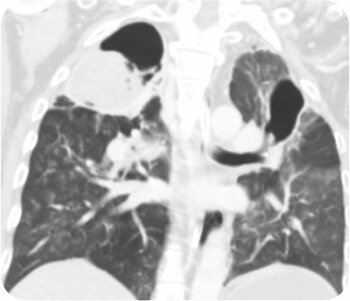
CT chest was suggestive of cavity in left upper lobe. FOB was suggestive of pus oozing from left upper lobe bronchus with a clot mass adherent to left upper lobe bronchus. Subsequent bronchoalveolar lavage was predominantly neutrophilic. Staining and culture for pyogenic, fungus, tuberculosis and nocardia was negative. Cytology was negative for malignancy. A diagnosis of Invasive Mucormycosis was made.
Rigid bronchoscopy + Cryobiopsy of protruding mass + Endobronchial blocker ( Fogarty balloon) was done.
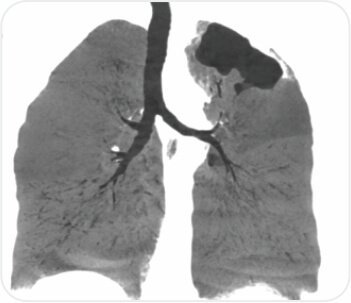
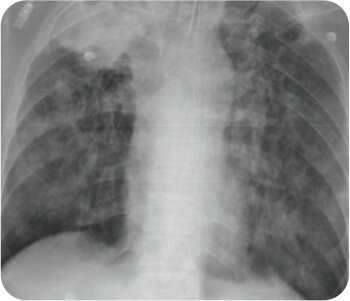
CT chest – cavity in left upper lobe
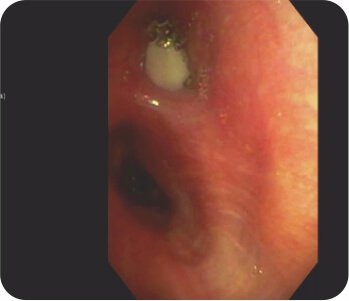
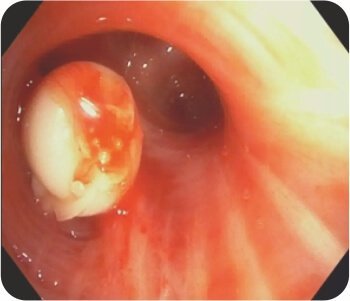
Bronchoscopy – Pus oozing from left upper lobe bronchus
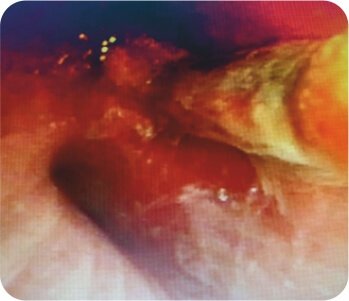
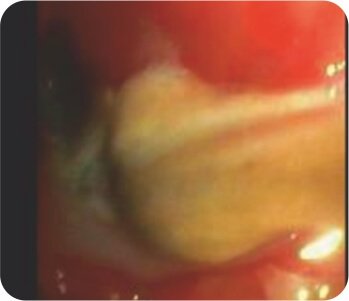
Bronchoscopy – Mass/ Clot occluding the left upper lobe bronchus
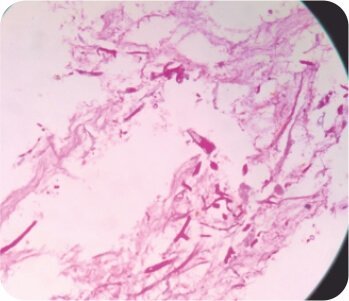
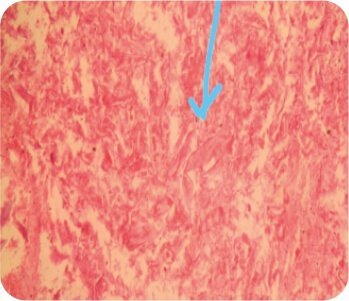
Cryobiopsy of the protruding mass suggestive of invasive mucor mycosis (Broad aseptate hyphae)
About Author –
Dr. Viswesvaran Balasubramanian, Consultant Interventional Pulmonology and Sleep Medicine, Yashoda Hospital, HyderabadMD, DNB, DM (Pulmonary-Gold Medal), Fellowship in Sleep Medicine (Gold Medalist), Fellowship in Interventional Pulmonology (Malaysia)
Bronchial Artery Embolisation and Sphigot Insertion of Bronchus
Background
50 year old alcoholic patient presented with massive hemoptysis. Patient was intubated in emergency for need of airway protection.
Diagnosis And Treatment
CT chest with thoracic angiogram revealed bilateral cavitary lesion with hypertrophied collateral arteries predominantly supplying the right upper lobe cavity. FOB done showed active bleeding from right upper lobe bronchus.
Watanabe sphigot occlusion of anterior subsegment of right upper lobe + glue instillation of right apical and posterior sub segment followed by bronchial artery embolization was done.

Pre procedure CT Scan
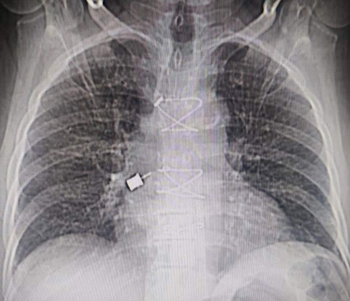
Pre procedure X ray
Pre procedure CT Scan
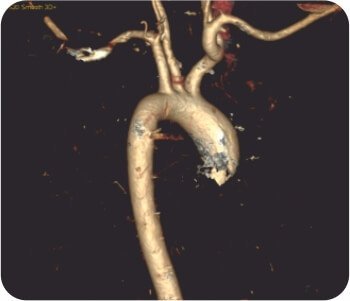
CT thoracic angiograph

Active hemoptysis
Placement of sphigot in right upper bronchus
Placement of sphigot in right upper lobe bronchus

Glue instillation in right upper lobe bronchus
About Author –
Dr. Viswesvaran Balasubramanian, Consultant Interventional Pulmonology and Sleep Medicine, Yashoda Hospital, HyderabadMD, DNB, DM (Pulmonary-Gold Medal), Fellowship in Sleep Medicine (Gold Medalist), Fellowship in Interventional Pulmonology (Malaysia)
FOREIGN BODY REMOVAL- DENTAL HEX DRIVER
Back ground
' The Fleeting foreigner ' ,80 year old , male, non smoker
C/o :
DM, HTN, CAD - Dual antiplatelet therapy
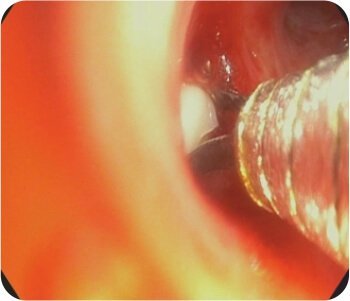
Accidental aspiration of ' Dental HEX driver - Metallic foreign body ' during dental procedure
Procedure :
Foreign body removal - Dormia basket


Learning points
- Metallic foreign bodies are slippery and may be difficult to grasp with forceps
- CXR immediately prior to procedure is desired as position of foreign body may change with cough
- Early identification and removal avoids post obstructive pneumonia or stenosis
- The key sign that most dentists recognize when patients aspirate an object during a dental procedure is coughing.
- Assessment of parts of instruments should be done promptly with a high degree of suspicion for possible swallowing or aspiration if an object is missing.
About Author –
Dr. Viswesvaran Balasubramanian, Consultant Interventional Pulmonology and Sleep Medicine, Yashoda Hospital, HyderabadMD, DNB, DM (Pulmonary-Gold Medal), Fellowship in Sleep Medicine (Gold Medalist), Fellowship in Interventional Pulmonology (Malaysia)
In case of any pulmonary issues, consult right away